
Does socioeconomic environment pose as a risk factor for malaria in Senegal? A DHS data analysis of malaria trends from 2010 to 2016 in Senegal
Ndèye Marème Sougou, Adama Faye, Mamadou Makhtar Mbacké Leye, Oumar Bassoum, Ibrahima Seck
Corresponding author: Ndèye Marème Sougou, Department of Preventive medicine and Public Health, University Cheikh Anta Diop, Dakar, Senegal 
Received: 13 Oct 2021 - Accepted: 06 Jan 2022 - Published: 01 Apr 2022
Domain: Environmental health,Public health,Malaria control program
Keywords: Trend of malaria, associated factors, Senegal
©Ndèye Marème Sougou et al. PAMJ-One Health (ISSN: 2707-2800). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Ndèye Marème Sougou et al. Does socioeconomic environment pose as a risk factor for malaria in Senegal? A DHS data analysis of malaria trends from 2010 to 2016 in Senegal. PAMJ-One Health. 2022;7:28. [doi: 10.11604/pamj-oh.2022.7.28.32017]
Available online at: https://www.one-health.panafrican-med-journal.com/content/article/7/28/full
Research 

Does socioeconomic environment pose as a risk factor for malaria in Senegal? A DHS data analysis of malaria trends from 2010 to 2016 in Senegal
Does socioeconomic environment pose as a risk factor for malaria in Senegal? A DHS data analysis of malaria trends from 2010 to 2016 in Senegal
Ndèye Marème Sougou1,2,3,&, Adama Faye1,2, Mamadou Makhtar Mbacké Leye1,2, Oumar Bassoum1,2, ![]() Ibrahima Seck1,2
Ibrahima Seck1,2
&Corresponding author
Introduction: in Senegal, many interventions have been carried out in the fight against malaria. Thus, the prevalence of malaria has clearly declined from 2010 to the present day. The analysis of the evolution of malaria will aid in addressing the determinants of malaria elimination in this country. The purpose of this research is to analyze the evolution of malaria in Senegal from 2010 to 2016.
Methods: data from the Senegal Demographic and Health Surveys (for 2010-2011, 2012-2013, 2014, 2015, and 2016) are used in this article. Malaria prevalence had been studied on the basis of RDT positivity. A multivariate logistic analysis with an adjustment over the years was performed to identify the factors associated with the evolution of malaria in Senegal. The adjusted odds ratios were calculated with their 95% confidence intervals. The dependent variable was the result of the malaria rapid diagnostic test.
Results: the prevalence of malaria ranges from 3.01% in 2010 to 0.87% in 2016. The age of the child 4 years (aOR=1.82 [1.14-2.89]) and 5 years (aOR=1.98 [1.21-3.25]) were risk factors associated with the evolution of malaria. With an aOR of 0.02 [0-0.18], the richest wealth quintile was a protective factor against malaria. The characteristics of house constructions were also protective factors against malaria. These are houses with improved wall and roof materials, and their aOR are 0.45 [0.24-0.85] and 0.48 [0.25-0.93], respectively.
Conclusion: the age of the children, the level of wealth in the household, and the type of dwelling in the house are all factors associated with the evolution of malaria in Senegal. It should be noted that a country's level of development, which influences better living conditions for communities, remains an important prerequisite for the eradication of malaria in the African subregion, and particularly in Senegal.

Since the 1950s and 1960s, the international community has prioritized the fight against malaria and its eventual eradication [1,2]. However, Africa continues to be the epicentre of this endemic. Due to a lack of resources as a result of the global malaria eradication plan´s halt (UNICEF and other donors having withdrawn their financial contributions), the disease has been completely neglected for decades, resulting in the resurgence of malaria in areas where it had been reduced, with outbreaks leading to high mortality [3,4]. About 95% of malaria deaths globally were in 31 countries. Nigeria (23%), the Democratic Republic of the Congo (11%), the United Republic of Tanzania (5%), Mozambique (4%), Niger (4%) and Burkina Faso (4%) accounted for about 51% of all malaria deaths globally in 2019 [5]. It should be noted, however, that in recent years, some countries in sub-Saharan Africa have significantly reduced malaria prevalence and in some regions are in elimination (Algeria and Cabo Verde, since 2019), while other countries in sub-Saharan Africa continue to have high malaria endemicity [5].
Malaria incidence has decreased dramatically in Senegal in recent years, dropping by more than 50% between 2009 and 2015. Between 2009 and 2014, parasite prevalence decreased from 3 to 1.2%, and all-cause mortality decreased from 72% of live births to 33% among children under 5 years of age. Senegal was able to meet the Rollback Malaria targets in 2015 owing to these convincing results [4]. Several studies have shown that the risk of malaria infection is related to a country´s level of development. For example, the risk of malaria infection has been linked to the level of household wealth [6,7]. According to research, the quality of housing construction is also an important risk factor for malaria [8]. Some of the factors identified in the scientific literature may imply that, despite health interventions, malaria elimination in sub-Saharan Africa would be difficult to achieve because of country´s level of development. The aim of this study is to analyze the evolution of malaria in Senegal from 2010 to 2016.

Data
This article uses data from the Senegalese Demographic and Health Surveys (DHS) (e.g Demographic and Health Surveys (DHS)) for 2010-2011, 2012-2013, 2014, 2015 and 2016. The DHS sample is representative at the national, regional, urban, and rural levels, as well as at the level of the 14 regions of Senegal. The DHS sample is drawn stratum by stratum. Thus, the sample is based on a stratified, two-stage, areal sample drawn in accordance with the DHS sampling methodology [9]. At the first level, the DHS in Senegal covers 400 clusters (Primary Survey Units PSU) drawn from a list of Enumeration Zones established during the General Census of Population and Housing, Agriculture and Livestock, using a systematic draw with probability proportional to size, with the size of the UPS being the number of households [9]. A count of households in each of these clusters provides a list of households from which a second-stage sample of 22 households per cluster was drawn, in both urban and rural areas, using a systematic draw with equal probability. In 2010-2011, 7,902 households were surveyed; in 2012-2013, 4,131 households were surveyed; in 2014, 4,231 households were surveyed; and in 2015, 4,511 households were surveyed by DHS.
Malaria parasitemia tests were performed during these surveys. Malaria parasitemia tests were carried out on children aged 6 to 59 months. A Rapid Diagnostic Test (RDT), the results of which were communicated to the parents/caregiver, and a thick drop were used to diagnose malaria. According to the protocol in place, children who tested positive on the RDT were referred to a health service by survey laboratory technicians. The RDT results are used in this study.
Dependent variable
The dependent variable was the existence of malaria. The result of the rapid diagnostic test was used for the diagnosis of malaria. This variable is a binary DHS variable which has 2 modalities "positive" and "negative".
Independent variables
The study considered explanatory variables related to socio-economic and demographic factors. These included individual factors, household factors, and factors related to means of prevention. With respect to (A) individual factors: 1) age was analyzed by 1-year age group; 2) sex was a 2-modality binary variable; 3) the variable "Child works on a farm or with animals" was also binary; (B) household factors: 1) household wealth - the wealth index, a measure of relative economic well-being based on household assets, was ranked by quintiles (lowest, second, middle, fourth, and highest); 2) residence - the place of residence has been dichotomized into "urban" or "rural"; 3) the construction material of the houses with the following variables - "Main wall material (wall)" was generated from an EDS variable with 14 modalities: no walls, cane/palm/trunks, dirt, bamboo with mud, stone with mud, adobe uncovered, plywood, cardboard, reused wood, cement, lime stone / cement, bricks, cement blocks, adobe covered (Adobe is sun-hardened brick, made from mainly clay soil, diluted and mixed with straw or chopped dry grass), wood planks / shingles, etc. This was recoded into 2 modalities "improved material" and "unimproved material". The "improved material" modality corresponded to the modalities, cement, limestone / cement, bricks, cement blocks, adobe coated, and wood planks / shingles. The variable "Main roof material" was generated from an EDS variable with the following 12 modalities: no roof, stubble/palm leaves, grass, rustic carpet, palm/bamboo, wood planks, cardboard, metal, wood, scale/cement fibre, ceramic, cement and roof shingles. This was recoded into a binary variable with two modalities: "improved material" and "unimproved material". The "improved material" modality corresponded to the metal, wood, cement fibre/calamine, ceramic, cement and roofing shingles modalities.
The variable "main soil material" was recorded from the EDS variable with the modalities: "earth, sand", "manure", "wood planks", "palm, bamboo", "parquet, polished wood", "vinyl, asphalt strips", "ceramic tiles", "cement", "carpet" and others. This variable was recoded as "improved material" and "unimproved material". The enhanced material modality was "parquet, polished wood", "vinyl, asphalt strip", "ceramic tile", "cement", and "carpet".
Concerning the (C) factors relating to means of prevention concerns the following variables: (1) The variable "existence of windows with mosquito nets in the house" had 2 modalities "yes" and "no". (2) The variable "child sleeps under mosquito nets all night" was generated from a variable "Children under 5 years who slept under mosquito nets last night". This variable had 4 modalities "no", "all children", "some children", and "no nets in the household". The variable was recoded into a binary variable with two modalities "yes" and "no", the "yes" modality corresponded to children having "slept under a net last night". (3) The variable "use of mosquito nets as a means of prevention outside sleeping rooms" was also binary.
Analysis
STATA/SE 15.1 software was used for the analysis. Using the STATA append function, we combined the EDS surveys from 2010-2011, 2012-2013, 2014, 2015, and 2016. A two-stage sampling design was used, as earlier mentioned in the section on data sources. All data were weighted to account for disproportionate sampling and non-response to account for the survey's multi-stage sampling design. The variables in the descriptive analysis were presented in terms of frequency and percentage of data. Inter-group comparisons were made using the Chi2 test. The significance level was set at 5, and 95% confidence intervals (CI) were used. Variables where p was less than 0.2 in the bivariate analysis were selected for the multivariate analysis [10].
A multivariate logistic analysis was performed to account for the effect of confounding factors in assessing the factors associated with the positivity of the RDT. The 95% confidence intervals for adjusted odds ratios (adjusted odd ratio (ORa)) were calculated. Before using the svy command to handle complex sampling (multi-stage sampling, weighting, and stratification), the identification variables for weights, strata, and primary sampling units (PSUs) were defined (survey prefix STATA). The logistic model was fitted using the previously mentioned independent variables.
Participants
A secondary analysis of Senegal DHS data (2010-2016) was carried out in our study. Participants were drawn from Senegal's 14 administrative regions, both urban and rural. The study focused on the use of rapid diagnostic tests (RDTs) to diagnose malaria in children under the age of five. Our study included 408 969 children over the course of five years. Figure 1 depicts the flow diagram of the study population.
Sociodemographic characteristics
From 2010 to 2016, more people lived in rural areas than in the countryside, with rural areas accounting for 55.13% of the population in 2010 and 54.54% in 2016 (Table 1). We see an improvement in the construction of houses with improved roofing materials, leaving the rate of 76.36% to represent 81.62% of houses in 2016 (Table 1). The percentage of houses with improved floor construction equipment increased from 65.99% in 2010 to 77.11% in 2016 (Table 1). From 2010 to 2016, the percentage of houses with improved wall construction material remained relatively constant. It increases from 70.1% in 2010 to 70.91% in 2016. In terms of prevention methods, the number of children increased from 23.41 to 46.28%, respectively between 2010 and 2016 (Table 1). Use of mosquito nets outside sleeping rooms increased from 24.45% in 2010 to 30.47% in 2016. The percentage of houses with mosquito nets on their windows increased from 14.85% in 2010 to 23.67% in 2016 (Table 1).
Evolution of malaria cases from 2010 to 2016
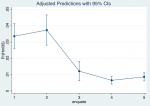
The malaria prevalence rate varies from 3.01% in 2010 to 0.87% in 2016 (Table 2). In survey 2, which corresponds to the years 2012-2013, the evolution of malaria cases shows an increase. This results in a significant and consistent decrease until 2016 (Figure 2).
Associated factors with the evolution of malaria in Senegal from 2010 to 2016
The age of the child is one of the risk factors associated with the progression of malaria. Children aged 4 and 5 are 1.82 times (aOR=1.82 [1.14-2.89]) and 1.98 times (aOR=1.98 [1.21-3.25]) more likely to have malaria, respectively (Table 3). The richest wealth quintile is associated with the evolution of malaria. It is a protective factor against malaria with aOR=0.02 [0-0.18] (Table 3). The construction characteristics of the houses are also protective factors against malaria. These are houses with better wall and roof materials, with aORs of 0.45 [0.24-0.85] and 0.48 [0.25-0.93], respectively (Table 3).
Malaria trend in Senegal from 2010 to 2016
Globally, the number of malaria cases is estimated at 228 million in 2018 (95% confidence interval (CI): 206-258 million), up from 251 million in 2010 (95% CI: 231-278 million) and 231 million in 2017 (95% CI: 211-259 million). The WHO African Region recorded the greatest number of cases (213 million, or 93%) in 2018. Nineteen sub-Saharan African and Indian countries accounted for nearly 85% of all malaria cases worldwide. Nigeria (25%), the Democratic Republic of the Congo (12%), Uganda (5%), Côte d'Ivoire (4%), Mozambique (4%), and Niger are the six African countries that have recorded more than half of the cases (4%) [11]. However, as of 2016, the World Health Organization had identified 21 countries with the potential to eliminate malaria by 2020. WHO is collaborating with the governments of these "E-2020" countries to help them meet their elimination goals [11]. According to this study, Senegal has a malaria prevalence of 0.87%, putting it among the countries with the greatest potential for elimination.
Malaria prevalence in Senegal increased slightly from 3.01 to 3.65% between 2010 and 2013, according to an analysis of the evolution of the disease. Malaria prevalence will gradually decline beginning in 2013 and reaching 0.87% in 2016. Despite its proximity to some West African sub-regional countries, Senegal has made significant progress in lowering its malaria prevalence rate. Despite having similar Sudano-Sahelian climates, these neighboring countries have higher malaria prevalence than Senegal. This is the case for Nigeria (27%) and Niger (3%) for malaria cases [5]. For deaths due to malaria, this is the case for Nigeria (23%), Burkina Faso (4%) and Niger (4%) [5]. According to the RDT, the prevalence of malaria in Mali is 19% [12], in Guinea Conakry 26% of children have been treated for malaria [13], and in Burkina Faso, the prevalence of malaria is 17% [14].
Some other countries in Africa region achieve the malaria elimination. It´s the case for Algeria which is certified malaria free by WHO in 2019 and Cabo Verde [5]. Senegal's low prevalence could be attributed to the country´s malaria-fighting policies. In fact, many interventions are being implemented in Senegal, including chemo-prevention of seasonal malaria, universal coverage with impregnated mosquito nets, and intermittent preventive treatment for pregnant women. For children living in areas of the Sahel where malaria transmission is highly seasonal, chemoprevention with sulfadoxine-pyrimethamine plus amodiaquine, administered monthly during the transmission season, is recommended. The recommendation for chemoprevention of seasonal malaria is currently limited to children under five years of age, but in many areas of seasonal transmission, the burden of older children may justify an extension of this age limit. Chemoprevention was introduced in Senegal in 2008 and made available in all districts by 2010. In Senegal, evaluations of its effectiveness revealed that the introduction of seasonal chemoprevention of malaria in children was effective and associated with a reduction in malaria incidence overall [15,16].
Other prevention measures recommended by the World Health Organization (WHO) in endemic areas to reduce malaria-related morbidity and mortality include vector control through the provision and use of insecticide-treated nets (e.g. insecticide-treated nets (ITNs)) and intermittent preventive treatment during pregnancy (intermittent preventive treatment (IPT)) to prevent malaria associated with pregnancy [17]. Since 2011, Senegal has extended national ITN distribution to the entire population through various channels such as health centers, community organizations, schools, and social marketing activities [18]. However, according to the results of successive demographic and health surveys, the level of use of IPT and ITNs in Senegal is higher in the 2013-2014 DHS than in previous years: in 2009, IPT use was 12%, and in 2010 it rose to 39% [19]. This could explain the acceleration of the curve of the decline of malaria that is noticed by our study. According to studies, the adoption of malaria prevention methods (IPT and ITNs) in Senegal has been effective in the fight against malaria [20].
Associated factors with the evolution of malaria in Senegal from 2010 to 2016
Malaria morbidity is higher in children under the age of seven, according to studies [21]. The age of the child was found to be a factor in the progression of malaria in this study. Children aged 4 and 5 years were respectively 1.82 times (aOR=1.82 [1.14-2.89]) and 1.98 times (aOR=1.98 [1.21-3.25]) more likely to have malaria. Other studies have shown a correlation between the age of the child and the occurrence of malaria. In Malawi, children aged 4 were more likely to be infected with malaria, with an aOR=2.1; 95% CI: 1.3-3.3 [22]. This was also true in Burkina Faso, where children aged 4 and 5 were the most vulnerable, with an OR: 6.79 [5.62-8.22] [23]. This vulnerability of older children may be related to behavioral factors influencing the use of preventive measures in the 4-5 age group. Other studies had identified age as a factor associated with ITN use. Older children (5 years) were less likely to use ITNs (OR=0.37, 95% CI: 0.28-0.47) [24].
According to this study, the richest wealth quintile in Senegal is associated with the evolution of malaria. It has an aOR of 0.02 [0-0.18] for malaria protection. Several studies have found that socio-economic factors influence the occurrence of malaria. Thus, in several countries, including Burkina Faso and Pakistan, children in the poorest wealth quintile were more vulnerable to malaria than those in the richest wealth quintile [23,25]. The construction characteristics of the houses were also identified as protective factors against malaria in this study. These were houses with improved wall and roof materials with aOR 0.45 [0.24-0.85] and 0.48 [0.25-0.93] respectively. The results of our study were similar to those of a systematic review of studies evaluating the relationship between modern housing and malaria infection (n = 11 studies) and clinical malaria (n = 5 studies). According to the latter study, residents of modern homes were less likely to be infected with malaria than residents of traditional homes [8]. According to the 2015 study, future research should assess the protective effect of specific house characteristics and incremental housing improvements associated with socio-economic development.
As in our previous study in Nigeria, children who lived in houses built entirely of unimproved materials were more likely to be infected with malaria (aOR = 1.4, CI 1.08-1.80, p = 0.01). Our study was able to focus on improved wall and roof materials as protective factors against malaria, with aOR of 0.45 [0.24-0.85] and 0.48 [0.25-0.93], respectively.
This study concluded that the factors associated with the evolution of malaria in Senegal are the child´s age, the level of wealth of the household, and the type of dwelling in the house. Health policies in Senegal should prioritize the protection of children aged 4 to 5, who are particularly vulnerable to malaria infection. In addition to other malaria prevention strategies, educating Senegalese communities about the malaria-protective role of modern housing and encouraging the use of improved materials for house design (roof and wall) could help strengthen malaria control measures for children under the age of five. It should be noted that a country´s level of development, which influences better living conditions for communities, remains an important prerequisite for the elimination of malaria in the African sub region, and particularly in Senegal.
Limits
This study had some limitations that were discovered. These include differences in the specificity and sensitivity of the diagnostic methods (RDT and microscopy), as well as how the sampling strategy was carried out, which may have favored certain individuals in the population. Only the results of Rapid Diagnostic Tests were used in this study.
What is known about this topic
- WHO African Region recorded the greatest number of cases (213 million, or 93%) in 2018. Nineteen sub-Saharan African and Indian countries accounted for nearly 85% of all malaria cases worldwide;
- The quality of housing construction is an important risk factor for malaria.
What this study adds
- This study concluded that the factors associated with the evolution of malaria in Senegal are the child´s age, the level of wealth of the household, and the type of dwelling in the house;
- Health policies in Senegal should prioritize the protection of children aged 4 to 5, who are particularly vulnerable to malaria infection.
The authors declare no competing interests.
NMS analyzed and interpreted the data. AF proceeded to verify the statistical tests. AF, MMML and OB were major contributors in writing the manuscript. IS was major contributor in the manuscript. All authors read and approved the final manuscript.
Table 1: distribution of individual and household characteristics by year
Table 2: distribution of RDT-positive malaria cases from 2010 to 2016 in Senegal
Table 3: year-on-year adjustment of factors associated with the evolution of malaria from 2010 to 2016 in Senegal
Figure 1: study of diagram flow
Figure 2: evolution of malaria cases from 2010 to 2016 in Senegal
- WHO. Eighth World Health Assembly (Mexico, D.F., 10-27 May 1955). Official record of the World Health Organization, N°63. Geneva. 1955; pp 236-240.
- WHO. Expert Committee on malaria, sixth report, WHO technical report series, number 123. Geneva. 1957; 4 p.
- Nàjera JA, Gonzàlez-Silva M, Alonso PL. Some lessons for the future from the Global Malaria Eradication Programme (1955-1969). Plos One. 2011;8(1):e1000412. PubMed | Google Scholar
- Anderson DA. Eradication: lessons learnt from the past. Bulletin of the World Health Organization. 1998;76 Suppl 2(Suppl 2):17-21. PubMed
- World malaria report 2020. 20 years of global progress and challenges. Geneva. 2020. Licence: CC BY-NC-SA 3.0 IGO.
- Mfueni Bikundi E, Coppieters Y. Importance of risk factors associated with malaria for Sub-Saharan African children. Int J Environ Health Res. 2017 Oct;27(5):394-408. PubMed | Google Scholar
- Diallo A, Sié A, Sirima S, Sylla K, Ndiaye M, Bountogo M et al. An epidemiological study to assess Plasmodium falciparum parasite prevalence and malaria control measures in Burkina Faso and Senegal. Malar J. 2017 Feb 6;16(1):63. PubMed | Google Scholar
- Tusting LS, Ippolito MM, Willey BA, Kleinschmidt I, Dorsey G, Gosling RD et al. The evidence for improving housing to reduce malaria: a systematic review and meta-analysis. Malaria Journal. 2015 Jun 9;14:209. PubMed | Google Scholar
- USAID. Sampling and household listing manual. Accessed 11th Avril 2020.
- Collett D. Modelling binary data. Second edition. Accessed 9th Avril 2020.
- OMS. Le Rapport sur le paludisme dans le monde. 2019. Nombre de pages: 232. ISBN: 978-92-4-156572-1
- Ministère de l'Aménagement du Territoire et de la Population du Mali. Enquête Démographique et de Santé 2018. Mali 2018. Visité le 1er Mai 2020.
- République de Guinée. Enquête Démographique et de Santé 2018. Visité le 1er Mai 2020.
- Burkina Faso. Enquête sur les Indicateurs du Paludisme 2017-2018 (EIPBF). Visité le 1er Mai.
- Cissé B, Ba EH, Sokhna C, NDiaye JL, Gomis JF, Dial Y et al. Effectiveness of seasonal malaria chemoprevention in children under ten years of age in Senegal: a stepped-wedge cluster-randomised Trial PLoS Med. 2016 Nov 22;13(11):e1002175. PubMed | Google Scholar
- Ndiaye J, Ndiaye Y, Ba MS, Faye B, Ndiaye M, Seck A et al. Seasonal malaria chemoprevention combined with community case management of malaria in children under 10 years of age, over 5 months, in south-east Senegal: A cluster-randomised trial. PLoS medicine. 2019 Mar 13;16(3):e1002762. PubMed | Google Scholar
- WHO. Global technical strategy for malaria 2016-2030. Geneva. 2015. Accessed 9th Sept 20.
- Programme National de Lutte contre le Paludisme. Plan stratégique national de lutte contre le paludisme 2016-2020. 2013. Accessed 1er Mai 2020.
- United State Agency for International Development. Sénégal Enquête démographique et de Sante continues 2012-2014. Accessed 1er Mai 2020.
- Mouhamed Abdou Salam Mbengue, Amy Bei K, Aminata Mboup, Ambroise Ahouidi, Moussa Sarr, Souleymane Mboup et al. Factors influencing the use of malaria prevention strategies by women in Senegal: a cross-sectional study. Malaria Journal. 2017;16(1):470. PubMed | Google Scholar
- Greenwood BM, Bradley AK, Greenwood AM, Byass P, Jammeh K, Marsh K et al. Mortality and morbidity from malaria among children in a rural area of The Gambia, West Africa. Trans R Soc Trop Med Hyg. 1987;81(3):478-86. PubMed | Google Scholar
- Zgambo M, Mbakaya BC, Kalembo FW. Prevalence and factors associated with malaria parasitaemia in children under the age of five years in Malawi: A comparison study of the 2012 and 2014 Malaria Indicator Surveys (MISs). PLoS One. 2017;12(4):e0175537. PubMed | Google Scholar
- Ouédraogo M, Samadoulougou S, Rouamba T, Hien H, Sawadogo JEM, Tinto H et al. Spatial distribution and determinants of asymptomatic malaria risk among children under 5 years in 24 districts in Burkina Faso. Malar J. 2018;17(1):460. PubMed | Google Scholar
- Tchinda VHM, Socpa A, Keundo AA, Zeukeng F, Seumen CT, Fomban Lek RG et al. Factors associated to bed net use in Cameroon: a retrospective study in Mfou health district in the Centre Region. Pan African Medical Journal. 2012;12:112. Epub 2012 Aug 31. PubMed | Google Scholar
- Asif AM, Tahir MR, Arshad IA. Socioeconomic condition and prevalence of malaria fever in Pakistani children: findings from a community health survey. J Trop Pediatr. 2018;64(3):189-194. PubMed | Google Scholar
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures

Article metrics

