
Public health surveillance system evaluation: case of rabies surveillance in Burayu Town, Oromiya, Ethiopia, 2019
Fufa Hunduma, Belayneh Leulseged
Corresponding author: Fufa Hunduma, Saint Paul's Hospital Millennium Medical College (SPHMMC), Addis Ababa, Ethiopia 
Received: 28 Feb 2020 - Accepted: 13 Dec 2020 - Published: 15 Jan 2021
Domain: Environmental management,Epidemiology,Infectious diseases epidemiology
Keywords: Rabies, surveillance system evaluation, Burayu
©Fufa Hunduma et al. PAMJ-One Health (ISSN: 2707-2800). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Fufa Hunduma et al. Public health surveillance system evaluation: case of rabies surveillance in Burayu Town, Oromiya, Ethiopia, 2019. PAMJ-One Health. 2021;4:5. [doi: 10.11604/pamj-oh.2021.4.5.22048]
Available online at: https://www.one-health.panafrican-med-journal.com/content/article/4/5/full
Research 
Public health surveillance system evaluation: case of rabies surveillance in Burayu Town, Oromiya, Ethiopia, 2019
Public health surveillance system evaluation: case of rabies surveillance in Burayu Town, Oromiya, Ethiopia, 2019
![]() Fufa Hunduma1,&, Belayneh Leulseged2
Fufa Hunduma1,&, Belayneh Leulseged2
&Corresponding author
Introduction: public health surveillance is ongoing, systematic collection, analysis, interpretation, and dissemination of data regarding a health-related event for use in public health action to reduce morbidity and mortality and to improve health. In Ethiopia, 20 diseases and conditions are selected to be included in routine surveillance that reported immediately or weekly. Rabies is among immediately reportable disease. This study aims to evaluate the existing surveillance system of rabies in Burayu Town, Oromiya regional state.
Methods: this surveillance system evaluation was conducted in Burayu Town, Oromiya region by cross-sectional study design. Data was collected from Burayu Health Office, three Health centers, and five Health Posts using standard questioner prepared for public health surveillance system evaluation from January 15-30, 2019. Data were analyzed by MS. Excel.
Results: Burayu town has 302,543 population; all are at risk of rabies. The rabies surveillance system is being conducted regularly and consistently in the town. It captured 452 cases over the last four and half years, among them 267 (59.1%) were confirmed to be positive by laboratory investigation. It was useful, flexible, simple, sensitive, and stable. However, resources are poor, supervision and feedback are also intermittent and not regular. Epidemic preparedness and response team is not established at health facilities and planning for the surveillance is not practiced.
Conclusion: the surveillance system is functioning persistently, but regular supervision and feedback, availing case definitions and guidelines should be ameliorated. A written plan preparation by health facilities regarding the surveillance system, document keeping, resource planning and data analysis requires improvement.

Public health surveillance is the ongoing, systematic collection, analysis, interpretation, and dissemination of data regarding a health-related event for use in public health action to reduce morbidity and mortality and to improve health. A well-performing disease surveillance system is very important to the health system in providing evidence-based information for planning, implementation, monitoring, and evaluation of public health intervention programs. Effective communicable disease surveillance systems are one of the basic strategies of national disease prevention and control [1,2]. During the 48th session of the World Health Organization Regional Committee for Africa, held in Harare in September 1998, member states adopted the Integrated Disease Surveillance (IDS) as a regional strategy for early detection for timely and efficacious response and action to priority communicable diseases [3]. In Ethiopia efforts to establish a disease surveillance system was initiated in 1947 when the government issued quarantine rules. Subsequently, several legal and administrative measures were taken to strengthen communicable disease surveillance [4]. In 1996, as part of the response to the growing public health problem with communicable diseases, Ethiopia introduced an integrated disease surveillance and response (IDSR) strategy focusing on 17 priority diseases. Since 2008 the FMoH launched a reform and restructuring of the health sector into different core processes, and in particular the disease surveillance and response with the concept of Business Process Reengineering (BPR) [3].
In Ethiopia, 21 diseases and conditions (14 are immediately reportable whereas 7 are weekly reportable) are selected to be included in the routine surveillance. Ensuring reliable reporting of surveillance data throughout the country is important so that program managers, surveillance officers, and other health care staff can use the information for action [3]. Surveillance system evaluation answers questions like does the system meet its objective? Is it useful for action takers and policymakers? And what measures could improve the performance and productivity of the surveillance system and the program(s) that it supports? [4]. Rabies is one of the immediately reportable diseases in Ethiopia [3]. It is a viral zoonotic encephalomyelitis transmitted to humans after exposure to infected mammals, mainly dogs, through bites, scratches, or licks on damaged skin or mucous membranes. This disease continues to represent a public health concern worldwide, with an estimate of 60,000 human deaths per year, mainly in low-income countries [5,6]. Because of limited control measures in many countries and a lack of governmental concern, rabies remains a neglected tropical disease [7,8]. According to Fekadu as sited by Reta et al. In Ethiopia, rabies remains to be one of the most feared infectious diseases and has been diagnosed for several years at the Ethiopian Public Health Institute. According to Deressa et al. as cited by Reta, available data during the years 2001 to 2009 at the institute showed that 35 to 58 annual human deaths were recorded mostly in Addis Ababa, the capital city of the country [5].
Public health surveillance systems should be evaluated periodically, and the evaluation should include recommendations for improving quality, efficiency, and usefulness [4]. Evaluation of a public health surveillance system focuses on how well the system operates to meet its purpose and objectives [1, 3]. In Ethiopia rabies is an important disease that has been recognized for many centuries and currently under public health surveillance [1,9]. Burayu town is one of the endemic towns in Ethiopia with enormous street dogs and wild animals like fox and hyena. Therefore evaluating public health surveillance systems is to ensure that problems of public health importance are being monitored efficiently and effectively. The objective here was to evaluate the existing surveillance system of rabies in Burayu, Oromiya.

Study area: this surveillance system evaluation was conducted in Burayu Town, Oromiya Region. Burayu is westward from the capital city Addis Ababa and has a total population of 102,543 according to the 2015 census projection (Figure 1). It has three health centers and four Health posts.
Study period: It was conducted from January 15 - 30, 2019.
Study design: cross-sectional study design by structured questionnaires was employed.
Source population: the source population was all health facilities serving people at risk of rabies in Burayu town, Oromiya.
Study population: the study population was all government health facilities that were serving people at risk of rabies that had been exposed to rabies and sought health care services in Burayu Town, Oromiya region.
Sampling techniques and sample size: whole take sampling technique was employed, a total of eight health facilities included, PHEM office of Burayu Town, three health centers, and four health posts.
Study unit: this evaluation was included in different governmental health facilities (Health centers and Health posts), and Burayu Town´s health offices.
Data collection methods: data was collected and documented by: performance of the core activities of the surveillance system of the town which includes case definitions, case detection, registration, reporting, data analysis, interpretation, dissemination, and epidemic preparedness and response; supportive activities of the surveillance system regarding supervision, staff training, information feedback, equipment (communication materials), and financial support were assessed; status of surveillance system attributes (sensitivity, positive predictive value, timeliness, simplicity, data quality, flexibility, usefulness, and acceptability) will be evaluated; these data were collected used by tools adopted from WHO and CDC tools which are designed for the assessment of communicable disease surveillance systems; posted flow charts of the surveillance system, graphs, tables, trends of rabies, availability of surveillance guidelines, standard case definition of rabies were checked; records of registration book, feedback reports of surveillance, weekly and immediate reports of surveillance in the past 3 months, line lists of outbreak investigation were reviewed regarding rabies and surveillance system as a whole; health professionals, focal persons of PHEM at a health facility level, PHEM officers at town´s health office interviewed by Semi-structured and structured questioner used to collect data.
Data analysis procedure: data was analyzed by graphs, tabulation, and quantitative and qualitative analysis employed by MS-Excel.
Case definition of rabies: a person bitten by a suspected mad dog or other animals.
Operational definition (attribute of surveillance system): acceptability: willingness of persons conducting surveillance and those providing data to generate accurate, consistent, and timely data; representativeness: the degree to which inference can be drawn from the information gathered by the surveillance system to the target population; reporting completeness: proportion of all expected reports in a reporting system that was actually received; reporting timeliness: proportion of all expected reports in a reporting system received by a given date (due date).
Data quality assurance: questionnaires or data collection tools were developed after thorough reviewing of the surveillance evaluation guideline of CDC and all questionnaires were administered by FETP residents to keep the consistency of administering the questions.
Calendar: Ethiopian calendar lags seven to eight years behind Gregorian Calendar (G.C). From September to December it lags seven years and January to August lags eight years. It started in September and ended in August (Figure 2).
System description
Public health importance: currently, Burayu Town has a population of 302,543 with 51% male and 49% female population. It has three health centers and four Health posts. Burayu town was a rabies endemic area with all populations at risk of the disease. There was an enormous number of street dogs that increase the liability of the population of the town to rabies. Cases captured by the surveillance system were sent to EPHI for laboratory investigation and their result was collected (Figure 3). Those whose result turns to be positive and those who could not be determined start post-exposure prophylaxis by clinical decision. The trend of cases remained almost the same for the last four years, however environmental interventions to control street dogs relatively reduces the case in 2011 E.C/2018 (half of the year). In 2011 E.C (2018/2019) during the first six months, the reported 21 cases were relatively lower than the previous half years of data (Figure 4). As depicted in Figure 4, the cases were slightly increasing from 2008 to 2010 E.C. During the four and half years period there was a total of 452 cases captured by the surveillance system; among them, 267 (59.1%) turns to be positive by laboratory confirmation (Table 1).
Rabies reporting information flow: rabies reporting flow goes up from health post to health Centers, Burayu health office, Oromiya regional health bureau and finally reach Ethiopian Public Health Institute (EPHI). Usually, health centers send suspected cases directly to EPHI to get a confirmation by laboratory investigation, and Laboratory result sent directly to HC on request (Figure 5).
Core functions of the surveillance system
Case detection and registration: rabies cases were detected based on the case definition of rabies, however, the community's poor medical seeking behavior for rabies was identified as a factor that delays time interval between the presence of suspected animal and detection of the cases. All of the health facilities had clinical registries but there is a huge gap in keeping registrations and related documents appropriately. All of Health facilities had clinical register but none of them have rabies guidelines except Burayu Town´s health office PHEM. All had no rumor logbook for suspected outbreaks or events, no digitalized registration, and daily epidemic reporting format to regions.
Case confirmation: all health centers sent the head of dogs/animals to EPHI for laboratory confirmation of rabies cases and the result was available as needed. The suspected animal was taken to the EPHI and head cutting was done at the institution. When the result is needed, it is available immediately from the laboratory of EPHI.
Data reporting: despite rabies was classified as an immediately reportable disease, the surveillance system available was reporting the cases weekly. This comes from the poor application of daily reporting format and lack of sufficient training and poor awareness of the reporting schedule.
Epidemic preparedness and response: rapid response team (RRT) was established and functional at Burayu town health office but it was not functional and did not exist at health centers and health posts. At the town's health office, there was an emergency preparedness plan and rabies guideline but health centers and health posts had no guidelines and written plans. At all levels, there was no rabies surveillance training conducted over the last year, no budget allocated for rabies epidemic management and poor coordination between the veterinary department and human practitioners.
Outbreak investigation and confirmation: all levels of health facilities and Health office had specific written objectives for the rabies surveillance system. The main objectives of all health facilities and the town´s health office focused on the timely detection of a rabies outbreak. Fortunately, there was no recorded outbreak of rabies in the town over the last five years. Rabies case definition was not available at some of the health facilities, and all responded they have no capacity to collect specimens for a suspected rabid animal for laboratory diagnosis. All health facilities and the town´s health office believe that EPHI and regional PHEM would notify them of the laboratory result as soon as possible if an outbreak happens for further intervention.
Supervision: health centers responded they have not been supervised for the last two years.
Feedback: all health centers and health posts responded that feedback given from supervisors for them was poor and not regular, but Town´s Health office PHEM was given feedback intermittently from regional PHEM.
Data analysis and interpretation: all facilities said they analyzed the case of rabies but did not prepare in bulletin format for public and stakeholders use. On objective evaluation, there were no available analyzed results.
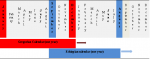
Resource (logistics and capacity building): generally, a resource for rabies surveillance was reported to be poor in all health facilities and the town´s health office. There was no budget allocated for rabies surveillance, a computer was available only at PHEM of health office, no vehicle and telephone was available specifically for surveillance. In addition to this, the main constraints for conducting rabies surveillance evaluation were reported to be the travel cost, unavailable per diem, training cost, and vehicle rent. Among documents that need to be available, PHEM guidelines, a written checklist for supervision, and case definition were available at the town´s health office but only outpatient registries were available at health facilities. Among formats needed to be available, the Weekly Report Form for Health Extension Workers (WRF-HEW), Weekly Disease Report Form (WDRF), and PHEM Case-based Report Form (CRF) was available at all health facilities and Town´s PHEM office (Table 2).
Credible evidence
Usefulness: all respondents believed that the surveillance of rabies was very useful because rabies had high public concern in the area. The process of surveillance was in status to solve health issues related to rabies and participants believed that it can detect the presence of an outbreak. Two health centers responded that they had used a surveillance system to monitor rabies morbidity and mortality trends in the population. All health facilities believed that surveillance can improve clinical practice regarding rabies detection and prevention. However, there was a lack of case definition in some health centers and health posts; the surveillance did not help in improving communication between stakeholders. Reporting formats lack important variables like age, sex, address which might help for further study.
Assessment of surveillance attributes
Simplicity: all participants agreed that the overall rabies surveillance system design and size were simple to use. Those who have rabies case definition said that it was easy to understand and it is helpful. It was not a burden to fill rabies reporting format and surveillance data management (entry, editing, analyzing, and storing) was simple. Even though respondents said high-level skill was not required to perform rabies surveillance system, they considered collecting rabies case information for reporting purpose was not an easy activity.
Acceptability: rabies surveillance was acceptable among stakeholders. Some health centers had no appropriate reporting formats during reporting but the town´s PHEM office had an appropriate one. Participation of the community into the rabies surveillance system was poor; they considered it was not their role to report rabies case and there was poor awareness about rabies surveillance in the community.
Flexibility: according to respondents the overall rabies surveillance system could easily be adapted to the user improvement demand. The ability to use different reporting mechanisms (SMS, phone call, paper format) and reporting format´s blank option could help to use for another surveillance system.
Timeliness: activities of rabies surveillance systems were conducted within a predefined time. Reports were regularly sent to a higher-level on time, and it was believed that no time delay would have happened between rabies outbreak notification and investigation in case it happened. Timeliness for the first and second quarters of this year was reported to be 74%.
Completeness: all reports that expected were done accordingly and for the last two quarters, it was 100%.
Representativeness: all population of the town was covered by this surveillance system.
Data quality: all participants believed rabies surveillance system generate quality data. There was regular feedback for towns PHEM office by a phone call from the Regional Health Bureau, and regular data check-up for rabies data quality. But no sufficient feedback, no adequate training on data handling, and reporting were given for health centers and health posts. Health centers and health posts are reporting the surveillance data on a weekly report format that is not appropriate and can diminish the quality of the data.
Stability: all participants believed that the rabies surveillance system was reliable respect to its stability. There were no circumstances that inhibited the surveillance system from operating appropriately. More than one person was available at Health centers for handling the surveillance system.
Predictive value positive: among 452 screened and captured cases 267 (59%) cases turn to be positive. Therefore predictive value positive of the surveillance system was 59%.
Communication: all health centers and PHEM officers submit a daily report by SMS, email, and phone call if the need arises. And usually submit a weekly report and monthly report by email.
Procedure: the ability of the surveillance system to cut the head of the rabid animal for laboratory investigation was asked, and they responded that they send directly to EPHI for the procedure and communicate the result.
Once the symptom developed, rabies has a 100% fatality rate that it requires intensive action to control and eliminate the disease. To prevent rabies Ethiopia included under immediately reportable disease list of PHEM surveillance [10]. This study was conducted to see the strength and weaknesses of the rabies surveillance system at Burayu town, the Oromiya region. The system is functional and reporting flow goes up from health posts to the health center and finally reached the town´s health office. However, for laboratory investigation health centers directly send suspected cases to Ethiopian Public Health Institute (EPHI). The system is useful, timely, flexible, regular at all health facilities, and the town´s health office. Health centers can easily access the laboratory result of suspected cases from EPHI. The rabies epidemic preparedness and response team was established and regular supervision and feedback were conducted at the health office. However, at health facilities, there is no sufficient feedback, no regular supervision and training, no established rabies preparedness and response team and no guideline for rabies surveillance, and no written plan for surveillance and control of a possible outbreak. Data analysis was not being done due to the data was only collected by hard copy format and does not interred to an electronic database at health centers and health posts. This is similar to the study previously done at Gambella Regional state [11].
All attributes of the surveillance system are good, but data quality and timeliness require some improvement. Timeliness is one of the quality measures of the surveillance system and should be monitored regularly. It is a key element of the surveillance system that indicates the system's ability to take appropriate action on public health problems, based on the urgency and the type of responses needed [11]. Some health facilities reported to do analysis but no clear charts and graphs to show trends of rabies cases are available. The core functions of the surveillance system like recording, reporting, analysis, and feedback have to gap which have a negative implication on the quality of surveillance data. Surveillance data should have good quality because, without quality public health data, interpretation may mislead decision makers [12]. Generally, resources for rabies surveillance were scarce. The budget was not allocated specifically for rabies and no enough logistics and materials were available. Studies indicated that failure of surveillance systems in developing countries is usually due to limited available resources, lack of knowledgeable staff, disorganization, and poor infrastructure for finding and reporting cases [13].
No matter how the resources allocated for rabies surveillance were scarce, the surveillance system is ongoing and providing invaluable service for rabies related morbidity and mortality. We identified that regular supervision and feedback, availing case definitions and guidelines should be ameliorated. In addition to this, a written plan preparation by health facilities regarding the surveillance system, document keeping, resource planning and data analysis requires improvement.
What is known about this topic
- Rabies is zoonotic disease and once the symptoms manifested the fatality rate is 100%;
- The area is rabies endemic and the community is aware of the danger of rabies outbreak.
What this study adds
- Indicates the gap at financial planning and resource allocation at the health facilities for rabies surveillance;
- Identified weaknesses regarding timely reporting, data analysis and bulletin preparation.
The authors declare no competing interests.
FH: conceived the idea, wrote the proposal, supervised and conducted the data collection, data processing, analysis, and data interpretation, wrote the first draft, wrote the final paper and manuscript write-up. BL: reviewed and edited the paper, reviewed, and approved the final manuscript. All the authors have read and agreed to the final manuscript.
We are grateful to the Oromia Regional Health Bureau (ORHB) to allow us to access to the institutions and collect data we want. We also heartily thank Saint Paul´s Hospital Millennium Medical College for funding and technically supporting this evaluation.
Table 1: summary of rabies cases over the last four years. Indicates the number of cases captured by surveillance each year and the laboratory confirmation result
Table 2: summary of resources available for the surveillance system in public health facilities of Burayu Town. The table was constructed by the principal investigator based on the responses of health facilities
Figure 1: Burayu Town, special zone surrounding Finfinne, Oromiya Region. Created by principal investigator using ArcGIS version 10.4
Figure 2: comparison of Gregorian Calendar (E.C) with Ethiopian Calendar (E.C). Constructed by principal investigator based on Calendar of Ethiopia and Gregorian Calendar. Ethiopian new year starts in September and ends in August (blue horizontal bar)
Figure 3: shows the total number of cases captured by the surveillance system and laboratory results. Constructed by prinicipal investigator using Ms Excel
Figure 4: trends of cases for the last four years and a half. The trend remains almost the same over the duration of four years
Figure 5: direction of reporting flow and feedback. EPHI = Ethiopian public health institute, ORHB = Oromiya regional health bureau, HO=health office, HP=health post
- Getachew D. Ethiopia Field Epidemiology Training Program (EFETP) Compiled Body of Works in Field Epidemiology. (Thesis). Addis Ababa University. 2018; 71-80. Accessed February 20 2019.
- Gemechu S. Ethiopia Field Epidemiology Training Program (EFETP) Compiled Body of Works in Field Epidemiology. (Thesis). 2014. Accessed February 25 2019.
- Ibrahim A. Ethiopia Field Epidemiology Training Program (EFETP) Compiled Body of Works in Field Epidemiology. (Thesis). Addis Ababa University. 2016; 26-30. Accessed February 12 2019.
- Mikiyas T. Compiled body of works in field epidemiology, surveillance evaluation. Accessed January 29 2019.
- Reta T, Teshale S, Deressa HA, Mengistu M, Sifa D, Ali A et al. Rabies in animals and humans in and around Addis Ababa, the capital city of Ethiopia: a retrospective and questionnaire based study. Academic Journals. 2016;6(6):178-186. Google Scholar
- Léchenne M, Naïssengar K, Lepelletier A, Alfaroukh IO, Bourhy H, Zinsstag J et al. Validation of a rapid rabies diagnostic tool for field surveillance in developing countries. PLoS Negl Trop Dis. 2016 Oct 5;10(10):e0005010. PubMed | Google Scholar
- Jackson AC. Current and future approaches to the therapy of human rabies. Antiviral Res. 2013; 99(1):6-7. PubMed | Google Scholar
- Fooks AR, Banyard AC, Horton DL, Johnson N, McElhinney LM, Jackson AC. Current status of rabies and prospects for elimination. Lancet. 2014. Oct 11; 384(9951):1389-99. PubMed | Google Scholar
- Hamza KH, Deressa HA, Ahmed EY. Overview of rabies in and around Addis Ababa, in animals examined in EHNRI zoonoses laboratory between, 2003 and 2009. Ethiopian Veterinary Journal. 2010;14(4):91-101. Google Scholar
- Yosef W. Epidemiological Surveillance. Saint pauls Hospital Millennium Medical College. April 2015.
- Tesfa Fasil. Compiled body of work in FETP, surveillance system evaluation of Malaria. AAU, chapter three. Accessed April 2 2019.
- Ingrid Brigitte Weber. Evaluation of the notifiable disease surveillance system in Gauteng province, South Africa. Uninersity of Pretoria. 2007;(January). Google Scholar
- Center for Diseases Control and Prevention (CDC). MMWR updated guidelines for evaluating public health surveillance systems: recommendations from the guidelines working group. CDC. 2014;(July 2001). Google Scholar
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures



Article metrics

