
Coordinated response to anthrax outbreaks in the Upper East Region of Ghana; the role of One Health approach
Benjamin Obukowho Emikpe, Garba Maina Ahmed, Anthony Akunzule, Nii Nortey Hanson-Nortey, Peter Awin, Queenly Quartey, Henry Nii Ayi Anang, Augustine Agamba, Robert Bayuo, Ransford Okornor, Adongo Issifu Rahaman, Jeffery Elorm Akortia Agbemeetsi, Albert Agyapong Tweneboah, Derrick Adu Asare, Adelekan Oluseyi Okunlade, Evans Ayamdooh Nsoh, Fenteng Danso, Emmanuel Allegye-Cudjoe
Corresponding author: Benjamin Obukowho Emikpe, Department of Pathobiology, School of Veterinary Medicine, Kwame Nkrumah University of Science and Technology (KNUST), Kumasi, Ghana 
Received: 21 Oct 2023 - Accepted: 27 Feb 2024 - Published: 09 Apr 2024
Domain: Epidemiology, Public health emergencies, Health system development
Keywords: Anthrax, outbreak, One Health, Ghana, Upper East
©Benjamin Obukowho Emikpe et al. PAMJ-One Health (ISSN: 2707-2800). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Benjamin Obukowho Emikpe et al. Coordinated response to anthrax outbreaks in the Upper East Region of Ghana; the role of One Health approach. PAMJ-One Health. 2024;13:11. [doi: 10.11604/pamj-oh.2024.13.11.42004]
Available online at: https://www.one-health.panafrican-med-journal.com/content/article/13/11/full
Essay 
Coordinated response to anthrax outbreaks in the Upper East Region of Ghana; the role of One Health approach
Coordinated response to anthrax outbreaks in the Upper East Region of Ghana; the role of One Health approach
![]() Benjamin Obukowho Emikpe1,&, Garba Maina Ahmed2, Anthony Akunzule2,
Benjamin Obukowho Emikpe1,&, Garba Maina Ahmed2, Anthony Akunzule2, ![]() Nii Nortey Hanson-Nortey3, Peter Awin4, Queenly Quartey5, Henry Nii Ayi Anang6, Augustine Agamba7,
Nii Nortey Hanson-Nortey3, Peter Awin4, Queenly Quartey5, Henry Nii Ayi Anang6, Augustine Agamba7, ![]() Robert Bayuo6,
Robert Bayuo6, ![]() Ransford Okornor6, Adongo Issifu Rahaman6,
Ransford Okornor6, Adongo Issifu Rahaman6, ![]() Jeffery Elorm Akortia Agbemeetsi8,
Jeffery Elorm Akortia Agbemeetsi8, ![]() Albert Agyapong Tweneboah6, Derrick Adu Asare1,
Albert Agyapong Tweneboah6, Derrick Adu Asare1, ![]() Adelekan Oluseyi Okunlade9,
Adelekan Oluseyi Okunlade9, ![]() Evans Ayamdooh Nsoh10, Fenteng Danso11, Emmanuel Allegye-Cudjoe11
Evans Ayamdooh Nsoh10, Fenteng Danso11, Emmanuel Allegye-Cudjoe11
&Corresponding author
High morbidity and mortality from anthrax outbreaks threaten the economy and public health. Recent global recurrence has raised anthrax prevention, surveillance, and control concerns. This essay reports Ghana's anthrax outbreak and management with a focus on the geographical spread, containment, and response. The anthrax outbreak affected 13 Ghanaian districts in the Upper East of which 100 animals died including 51% sheep, 41% cattle, 6% goats, and 2% pigs. Collaboration between human health and veterinary professionals, private and international organizations, anthrax vaccines, and drone delivery shortened the devastating effects of the anthrax outbreak. The effective multiple sectoral and actors coordination, management, and response to the outbreak, could be a model for other countries for intra- and inter-One Health outbreak control collaborations.

Anthrax can kill humans and other warm-blooded animals [1,2]. Anthrax, caused by Bacillus anthracis, remains a global public health issue, especially in underdeveloped rural agricultural regions like West Africa [3]. Jones [4] says Bacillus anthracis thrives and reproduces in its host's circulatory system. The termination of its host and release via post-mortem bleeding allow it to spread to a new host in the environment. The anthrax bacterium produces long-lived soil-based spores. Anthrax spores can survive in the natural environment for almost a century and often live in animal burial sites [5]. There is evidence that anthrax spores can reinfect animals 70 years after disturbing burial sites containing infected animals [6].
Carlson et al. [7] report that anthrax outbreaks occur inconsistently around the world. Previous studies show that developing nations like Ghana have more anthrax outbreaks than developed nations [8,9]. Animal and human anthrax have been reported in Ghana. Blackburn et al. [9] reported 1,000 anthrax deaths in Ghana between 1980 and 2000. Most cases were in northern Ghana and were caused by infected cattle [9]. Human anthrax infection is usually oral, cutaneous, or pulmonary [10,11]. Human infection can occur through direct contact with domesticated livestock, hunting, slaughtering, and eating anthrax-infected carcasses [12,13]. According to Frankel et al. [10], anthrax can be contracted by inhaling or ingesting blood and other tissues from infected animals through broken skin. Direct exposure to animal fur, hide, or wool can also cause anthrax [10,11].
Anthrax outbreaks can cause high morbidity and mortality, putting the economy and public health at risk [14]. Recent global recurrence has increased attention to anthrax prevention, surveillance, and control [15,16]. This case study analyses an anthrax outbreak in Ghana from epidemiological, clinical, and public health perspectives. Ghana, in West Africa, has a diverse population and relies heavily on agriculture and livestock in May 2023. The above factors create an environment where infectious diseases like anthrax can spread quickly. Ghana has rarely had anthrax outbreaks. However, these outbreaks can have serious consequences, so timely and effective response strategies are needed [17]. This case report describes how public health, veterinary, environmental, local, and medical professionals collaborated to investigate and contain a recent anthrax outbreak. This paper analyses the Ghanaian anthrax epidemic investigation to improve our understanding of anthrax epidemiology, outbreak case management, and public health. This report also emphasises the importance of a multidisciplinary approach to zoonotic diseases and the urgency of mitigating infectious agent spread and its effects.
This essay described the May 2023 anthrax outbreaks in the Bansi community in Binduri, Upper East Ghana. Data on affected individuals, areas, and timeframes were used to assess outbreak extent, geographical spread, containment, and response. On June 2, 2023, Ghanaian health officials reported a possible anthrax epidemic in Binduri District, Upper East Region. The Upper East Regional Health Directorate of the Ghana Health Service received the first two cases, one of which was fatal, on June 1, 2023. After eating the cattle carcass on May 21, 2023, a 65-year-old man became ill and died on May 31, 2023, from suspected anthrax. The family buried him the same day. The second patient to consume the carcass was a young man with arm lesions on June 1, 2023. On the same day, he was taken to a private hospital in Bazua, Upper East Region, Ghana. The third suspected human anthrax case was a young man with cutaneous lesions and a swollen head. There were 13 suspected cases and one suspected anthrax death in Binduri on June 11, 2023. All 11 suspected patient samples tested negative for human anthrax at the Pong-Tamale Veterinary Laboratory.
Four cattle died in Bansi between May 20 and June 1, 2023, before human infections were reported. Over 100 people ate the first cattle carcass on May 21, 2023. The emergency health team burned the second cattle death on June 1, 2023. The third cattle death, which occurred around June 1, 2023, was sold to butchers against the veterinarian's advice, but the veterinary officers and district police retrieved the carcasses on June 2. On June 2, 2023, a bull slaughtered at Sapeliga in the Bawku West District and brought to Binduri was intercepted, blood samples were taken, and Pong Tamale Veterinary Laboratory found anthrax in the blood. On June 3, 2023, the fourth cattle died. Blood samples were taken, but the Fulani herdsman ignored the veterinarian's order to bury the carcass. The Bawku abattoir sold the carcass. But local measures got the carcass retrieved and buried properly. Pong Tamale Veterinary Laboratory found anthrax in the fourth carcass. Cases of anthrax in animals were identified through the use of a history of sudden death of animals, with unclotted blood oozing out from the orifices of the dead animals. Laboratory testing of sudden dead animal blood samples taken from the facial veins of the animals was used to confirm the presence of Bacillus anthracis. With regards to human suspected cases, blood samples of humans were collected and tested for the presence of the bacteria. The geographical distribution of the anthrax-affected districts is displayed in the geographical map shown in Figure 1. A total of 7 districts out of 15 in the Upper East Region were affected.
Animal anthrax death distribution by district: the results indicated a total of 100 deaths were recorded in districts in the Upper West and Upper East districts of Ghana. Out of these deaths, 41 were cattle, 51 were sheep, 6 were goats and 2 were pigs. Binduri recorded the highest number of deaths (9 cattle, 3 goats, 25 sheep, and 1 pig) in animals, followed by Garu (15 sheep and 2 cattle) and Bawku West (7 cattle, 2 goats, 3 sheep and 1 pig). The least number of deaths were recorded in Pusiga (1 sheep), Nabdam (1 cattle), and Tempane (1 cattle) as shown in Figure 2.
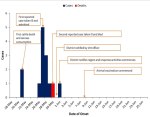
Human anthrax cases: a total of 13 cases were suspected, including one death. Out of the 13 suspected cases, 11 of the suspected case samples were taken to the laboratory. All 11 samples tested negative, as shown in Table 1. Between May 18 and June 26, 2023, the peak of cases was recorded on May 27, 2023, with five cases. The last suspected case was recorded on June 1, 2023 (Figure 3). The first cattle death and carcass consumption occurred on May 21, 2023, after which the subsequent deaths occurred from May 30, 2023, to June 5, 2023 (with the maximum number of cases being three). Animal vaccination, the ban on movement slaughtering, and the ban on the sale of animals commenced on June 7, 2023, and 3 cases were recorded on the said date as well. A few deaths were recorded between June 12 and June 13, 2023 (a maximum of two cases) after which no death was recorded until June 20, 2023, when 3 deaths were recorded.
The Government of Ghana, in collaboration with the Veterinary Service Directorate, Environmental Health, Ghana Health Service, and Local Government Agencies, implemented preventive measures in response to the anthrax epidemic. The implemented actions encompassed the establishment of veterinary units and laboratories equipped with the capacity to identify and manage instances of anthrax; alongside public awareness campaigns aimed at disseminating knowledge regarding preventive strategies. The transportation of animals into and out of the affected regions was banned, and the consumption of animal carcasses was forbidden. The official reaction encompassed several particular elements, including; i. The activation of the Regional Public Health Emergency Management Committee. This committee was responsible for coordinating various response operations and exhibited a notable level of involvement from the Regional Minister of the Upper East Region and political institutions. ii. Regional and District Rapid Response Teams were mobilized to conduct investigations into the epidemic. Furthermore, active case discovery and contact tracking measures were used. iii. In the region, a comprehensive prohibition was implemented on the transportation of animals (including cattle, sheep, goats, donkeys, and pigs) and their associated commodities for one month, commencing on June 7, 2023. iv. On June 7, 2023, a prohibition was implemented for one month, including the slaughtering, eating, and commercialization of both fresh and cooked animals. Additionally, all slaughterhouses within the specified territory were mandated to cease operations during this period. v. The management of suspected cases was commenced by administering antibiotics to all eleven (11) individuals. vi. The commencement of mass animal vaccination across all districts on June 6, 2023, was implemented as a preventive measure to curb the future dissemination of the epidemic throughout the animal population. As of June 8, 2023, a total of 2,339 ruminant animals, comprising 1,068 cattle, 757 sheep, and 514 goats, have received vaccination. As of June 11, 2023, a cumulative number of 16,800 cattle had been administered vaccinations. The vaccinations were deployed through drones as a means of expediting and addressing the urgent need to prevent a widespread outbreak of the illness at a national level. vii. Furthermore, there was an activation of heightened risk communication efforts in anticipation of the forthcoming Eid celebration.
Due to its hyper-endemicity and frequent outbreaks in West Africa, anthrax is underreported worldwide. This case report examined the recent anthrax outbreak in northern Ghana and the management strategy used to stop its spread. May to June 2023 was the duration of this anthrax outbreak. After a long dry season, Ghana's rainy season begins. Rains promote spring green-up and anthrax seasonality [7]. The anthrax outbreak affected 13 Northern Ghanaian districts, particularly the Upper East District. The 100 animals killed included 51% sheep, 41% cattle, 6% goats, and 2% pigs. The livestock distribution in the Upper East region where this outbreak occurred explains the higher anthrax rate in such livestock. Animal deaths were highest in Binduri, where the outbreak began. The Upper-East region has seen the majority of Ghana's anthrax outbreaks, with various districts affected, according to Blackburn et al. [9] and Awoonor-Williams [18].
Investigating herbal remedies used to cook anthrax-infected meat led to one death out of 13-suspected cases in Binduri. The butchering and eating of the anthrax-infected carcass caused many suspected human infections. This study and another by Opare et al. [19] confirmed the role of human behaviour, perceptions, and belief in human anthrax outbreaks. The infection may also spread due to improper carcass disposal [20]. Males outnumbered females in this outbreak of human anthrax. This supports previous outbreak reports by Awoonor-Williams et al. [18] and Blackburn et al. [9] that Upper East anthrax patients are mostly men. Men are more likely to be exposed to anthrax spores in infected animals because they slaughter and butcher them. Women cook the meat.
This outbreak lasted less than a month (from May 20, 2013, when the first cattle died to June 1, 2023, when the last suspected anthrax case was recorded). The shorter outbreak management time is due to human health and veterinary professionals working together, as seen during the COVID-19 pandemic. This coordinated approach may have been influenced by COVID-19 lessons. This may have led to the prompt 24-hour reporting to the appropriate authority, which activated the district-level emergency One-Health response team. After the regional emergency response unit was activated, anthrax vaccination, animal movement, slaughter, and sale bans began. The management and control of this outbreak are worthy of note because of the availability of the vaccine, the quick vaccine delivery using drones and the collective effort of human and animal health sectors with the involvement of private and international organizations hastened the process of the rapid response to dealing with this emergency outbreak. These private sector initiatives of vaccine delivery using drones were coordinated by Drone manufacturer, Zipline and technology pioneer Cowtribe who partnered with the Veterinary Service Department (VSD), Ministry of Health, and the Upper East Regional Coordinating Council (UER-RCC) to respond to the outbreak by distributing animal anthrax vaccine.
The international agencies which include FAO, WHO, UNHCR, and USAID promptly provided funds to facilitate the mobilization of the staff of VSD and the Ministry of Health in all these districts to combat the ravaging outbreak. The Regional Coordinating Council promptly coordinated the fund utilization in response to the outbreaks, while FAO led the joint field outbreak investigation using the One Health approach. In September 2023, FAO supported the Ghana Health Service in training its field staff as well as provided support to the Veterinary Services Directorate to organize an after-action review (AAR) to document lessons learned and the way forward with funding from the United States Agency for International Development (USAID). These interagency collaborations are very crucial for the mobilization of the veterinary staff to carry out vaccination, which enhances the coverage and control of outbreaks in Africa. The current anthrax outbreak in Ghana showed high case fatality in livestock, with a single death in humans. Despite this, the management and response involved a coordinated approach between several sectors and actors. This collective effort by the local authorities (VSD, MOH, UER-RCC), Private Sector (Zipline & Cowtribe), and international agencies (FAO, WHO, UNHCR, and USAID, among others) in the control of anthrax outbreak in the Upper East Region of Northern Ghana could serve as a model of intra and inter collaborations necessary for outbreak control using the One Health approach.

The authors declare no competing interest.
Benjamin Obukowho Emikpe conceptualized, designed, and drafted the article, Garba Maina Ahmed, and Anthony Akunzule conceptualized, acquired data, and reviewed the article critically for important intellectual content. Nii Nortey Hanson-Nortey, Peter Awin, Queenly Quartey, Henry Nii Ayi Anang, Augustine Agamba, Ransford Okornor, Adongo Issifu Rahaman, Jeffery Elorm Akortia Agbemeetsi, Albert Agyapong Tweneboah, Robert Bayuo aided in the acquisition of data and analysis of the data. Derrick Adu Asare drafted the article analysed and interpreted the data. Evans Ayamdooh Nsoh, Fenteng Danso, and Emmanuel Allegye-Cudjoe revised the article and provided some important information. All the authors have read and agreed to the final manuscript.
The authors would like to acknowledge the Veterinary Services Directorate of Ghana, the Ministry of Health, Ghana Health Services, the Environmental Protection Agency, The Ghana Police Service, and the leaders of the anthrax outbreak affected communities for their compliance and contribution to providing accurate data for this manuscript.
Table 1: distribution of human anthrax cases as of July 3, 2023
Figure 1: map of districts in the Upper East affected by anthrax (as of July 3, 2023)
Figure 2: animal anthrax death distribution by district
Figure 3: EPI curve of suspected cases of anthrax by the estimated date of onset - Binduri District, May 18 - June 26, 2023
- Chen WJ, Lai SJ, Yang Y, Liu K, Li XL, Yao HW et al Mapping the distribution of anthrax in mainland China, 2005-2013. PLoS Negl Trop Dis. 2016 Apr 20;10(4):e0004637. PubMed | Google Scholar
- Bakhteeva I, Timofeev V. Some peculiarities of Anthrax epidemiology in herbivorous and carnivorous animals. Life. 2022 Jun 10;12(6):870. PubMed | Google Scholar
- Carlson CJ, Kracalik IT, Ross N, Alexander KA, Hugh-Jones ME, Fegan M et al The global distribution of Bacillus anthracis and associated anthrax risk to humans, livestock and wildlife. Nature microbiology. 2019 Aug;4(8):1337-43. PubMed | Google Scholar
- Jones SD. Death in a Small Package: A short history of anthrax. Johns Hopkins University Press+ ORM; 2010 Oct 15. Google Scholar
- Norris MH, Kirpich A, Bluhm AP, Zincke D, Hadfield T, Ponciano JM et al. Convergent evolution of diverse Bacillus anthracis outbreak strains toward altered surface oligosaccharides that modulate anthrax pathogenesis. PLoS Biology. 2020 Dec 28;18(12): e3001052. PubMed | Google Scholar
- Finke EJ, Beyer W, Loderst�dt U, Frickmann H. The risk of contracting anthrax from spore-contaminated soil-A military medical perspective. European Journal of Microbiology and Immunology. 2020 Jun;10(2):29-63. PubMed | Google Scholar
- Carlson CJ, Getz WM, Kausrud KL, Cizauskas CA, Blackburn JK, Bustos Carrillo FA et al. Spores and soil from six sides: interdisciplinarity and the environmental biology of anthrax (Bacillus anthracis). Biological Reviews. 2018 Nov;93(4):1813-31. PubMed | Google Scholar
- Ohnishi N, Maruyama F, Ogawa H, Kachi H, Yamada S, Fujikura D et al. Genome sequence of a Bacillus anthracis outbreak strain from Zambia, 2011. Genome Announcements. 2014 May 1;2(2):10-128. PubMed | Google Scholar
- Blackburn JK, Kenu E, Asiedu-Bekoe F, Sarkodie B, Kracalik IT, Bower WA et al. High case-fatality rate for human anthrax, Northern Ghana, 2005-2016. Emerg Infect Dis. 2021 Apr;27(4):1216-1219. PubMed | Google Scholar
- Frankel AE, Kuo SR, Dostal D, Watson L, Duesbery NS, Cheng CP et al. Pathophysiology of anthrax. Front Biosci (Landmark Ed). 2009 Jan 1;14(12):4516-24. PubMed | Google Scholar
- Bayindir Y, Bayraktar M, Karadag N, Ozcan H, Kayabas U, Otlu B et al. Investigation and analysis of a human orf outbreak among people living on the same farm. New Microbiol. 2011 Jan;34(1):37-43. Epub 2011 Jan 15. PubMed | Google Scholar
- Ida JA. The biocultural landscape of zoonotic disease: Examining human-animal vulnerability to anthrax on the Colombian-Venezuelan border (Doctoral dissertation, University of Colorado at Boulder). 2016. Google Scholar
- Mwakapeje ER. Use of a One Health approach for understanding the epidemiology and management of anthrax outbreaks in the human-livestock-wildlife and environmental health interface areas of Northern Tanzania. 2019. Google Scholar
- Janik E, Ceremuga M, Niemcewicz M, Bijak M. Dangerous pathogens as a potential problem for public health. Medicina. 2020 Nov 6;56(11):591. PubMed | Google Scholar
- Mansingh A, Choudhary HR, Shandilya J, Bhattacharya D, Kshatri JS, Parai D et al. A qualitative exploratory study using One Health approach for developing an intervention package for elimination of human anthrax in an endemic district of Odisha, India. The Indian Journal of Medical Research. 2021 Mar;153(3):394. PubMed | Google Scholar
- Sarker MS, Shahid MA, Hoque MN, Sarker MA, Rahman MB, Islam SS. The The Rich Mapping: Be a Supplementary Approach for Anthrax Control at Community Level. Journal of Advanced Veterinary Research. 2021 Jan 6;11(1):41-6. Google Scholar
- Pittiglio C, Shadomy S, El Idrissi A, Soumare B, Lubroth J, Makonnen Y. Seasonality and ecological suitability modelling for anthrax (Bacillus anthracis) in Western Africa. Animals. 2022 Apr 29;12(9):1146. PubMed | Google Scholar
- Awoonor-Williams J, Apanga P, Anyawie M, Abachie T, Boidoitsiah S, Opare J et al Anthrax outbreak investigation among humans and animals in Northern Ghana: Case report. International Journal of TROPICAL DISEASE & Health. 2016 Jan 10;12(2):1-1. Google Scholar
- Opare C, Nsiire A, Awumbilla B, Akanmori BD. Human behavioural factors implicated in outbreaks of human anthrax in the Tamale municipality of northern Ghana. Acta tropica. 2000 Jul 21;76(1):49-52. PubMed | Google Scholar
- Nakanwagi M, Ario AR, Kwagonza L, Aceng FL, Mwesigye J, Bulage L et al. Outbreak of gastrointestinal anthrax following eating beef of suspicious origin: Isingiro District, Uganda, 2017. PLoS Negl Trop Dis. 2020 Feb 27;14(2):e0008026. PubMed | Google Scholar
Search
This article authors
On Pubmed
- Benjamin Obukowho Emikpe
- Garba Maina Ahmed
- Anthony Akunzule
- Nii Nortey Hanson-Nortey
- Peter Awin
- Queenly Quartey
- Henry Nii Ayi Anang
- Augustine Agamba
- Robert Bayuo
- Ransford Okornor
- Adongo Issifu Rahaman
- Jeffery Elorm Akortia Agbemeetsi
- Albert Agyapong Tweneboah
- Derrick Adu Asare
- Adelekan Oluseyi Okunlade
- Evans Ayamdooh Nsoh
- Fenteng Danso
- Emmanuel Allegye-Cudjoe
On Google Scholar
- Benjamin Obukowho Emikpe
- Garba Maina Ahmed
- Anthony Akunzule
- Nii Nortey Hanson-Nortey
- Peter Awin
- Queenly Quartey
- Henry Nii Ayi Anang
- Augustine Agamba
- Robert Bayuo
- Ransford Okornor
- Adongo Issifu Rahaman
- Jeffery Elorm Akortia Agbemeetsi
- Albert Agyapong Tweneboah
- Derrick Adu Asare
- Adelekan Oluseyi Okunlade
- Evans Ayamdooh Nsoh
- Fenteng Danso
- Emmanuel Allegye-Cudjoe
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures


Article metrics

